[NOTE: Anyone who has seen several derogatory articles about me on the web and is curious about what the real story is, please read this, this, and this.]
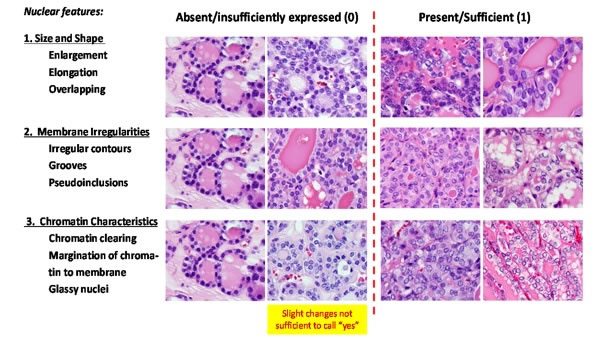
This is a panel showing some of the pathologic criteria for distinguishing invasive encapsulated follicular variant of papillary thyroid carcinoma from noninvasive. This is real science. Sayer Ji’s rant is not.
If there’s one lesson that we here at Science-Based Medicine like to emphasize, it’s that practicing medicine and surgery is complicated. Part of the reason that it’s complicated is that for many diseases our understanding is incomplete, meaning that physicians have to apply existing science to their treatment as well as they can. The biology of cancer, in particular, can be vexing. Some cancers appear to progress relentlessly, meaning that it’s obvious that all of them must be treated. Others, particularly when detected in their very early stages through screening tests, have a variable and therefore difficult to predict clinical course if left untreated. Unfortunately, some people, such as Sayer Ji, don’t understand that. They like their medicine black and white, and if physicians ever change guidelines in order to align them more closely with scientific understanding, they write blisteringly ignorant articles like ‘Oops… It Wasn’t Cancer After All,’ Admits The National Cancer Institute/JAMA.
Not exactly. An expert panel recommended reclassifying a specific thyroid lesion as not cancerous based on recent science. It’s called medicine correcting itself. Admittedly, this reclassification was probably long overdue, but what would Mr. Ji rather have? Medicine not correcting itself in this situation? In any case, when last I met Mr. Ji, he was happily abusing the science of genetics to argue that Angelina Jolie and other carriers of deleterious cancer-causing mutations don’t need prophylactic surgery because lifestyle interventions will save them through epigenetics, which to “natural health” enthusiasts like Mr. Ji seems to mean the magical ability to prevent any disease. Most recently, he has appeared on the deeply dishonest “documentary” about alternative medicine cancer cures The Truth About Cancer to expound on how chemotherapy is evil. His rant about the reclassification of a non-encapsulated follicular variant of papillary thyroid cancer as not cancer is more of the same, as you will see.
Overdiagnosis and the question of what is and isn’t “cancer”?
The sort of issue mangled by Mr. Ji in his article is one that those of us who treat breast cancer have been dealing with for a long time now. For example, as a breast cancer surgeon, I deal all the time with a disease entity known as ductal carcinoma in situ (DCIS). Basically, it’s a condition in which cancerous-appearing cells are found in the milk ducts of the breast but have not crossed the basement membrane, which is the membrane that surrounds the milk ducts. Generally, we consider DCIS to be stage 0 breast cancer, specifically cancer that hasn’t invaded through the basement membrane into the breast yet. Of course, as I’ve written before many times, it’s not as simple as that. Many—probably most—DCIS lesions never progress to cancer in the patient’s lifetime, particularly the so-called low grade lesions, which are called low grade because their cells resemble normal milk duct cells. On the other hand, higher grade lesions, which look more like frank cancer, likely progress to cancer at a much higher rate. However, because we have no reliable means of predicting which DCIS lesions will progress to invasive cancer and which will not, we end up treating them all in basically the same way: surgical excision plus or minus (usually plus) radiation plus or minus an estrogen-blocking drug.
Confusing the question of treatment of very early stage breast cancer is the apparent massive increase in incidence of DCIS over the last 40 years. Basically, as I’ve described multiple times before, the incidence of DCIS has increased 16-fold since 1975. Given that it’s highly implausible and unlikely that the “true” incidence of DCIS has increased so markedly in such a short time (and three or four decades is a short time for a change this massive), the likely explanation is the institution of widespread mammographic screening programs beginning in the early 1980s, leading to overdiagnosis.
Overdiagnosis is a phenomenon that’s been discussed here many times, both by myself and Harriet Hall. Basically, it is the detection of disease that would never go on to harm or kill the person harboring it. If there’s one thing that the mass screening of large asymptomatic populations for diseases has taught us, it’s that there’s a lot more preclinical disease out there in healthy people than we had previously suspected, or, as I put it, if you look very hard for a condition you will find more of it. Always. Indeed, thanks to a mass thyroid screening program after the Fukushima nuclear disaster, we recently learned that even children have way more preclinical thyroid cancer than we had previously thought. As I’ve discussed before, in autopsy studies half of men over 65 and three-quarters of men over 80 have tiny foci of cancer in their prostates; thyroid cancer can be found in 36% of adults, and the study’s investigators estimated that if the slices had been made thinly enough for microscopic examination they could have “found” thyroid cancer in close to 100% of adults between 50-70, even though clinically apparent thyroid cancer requiring treatment only has a prevalence in the population studied of around 0.1%. In breast cancer, it has been estimated that as many as one in three mammographically detected cancers in otherwise asymptomatic women might be overdiagnosed, although other estimates are around 10%. The reason the estimates vary so much is that we can’t do a study in which mammographically detected small invasive breast cancers are not treated is because, even if these estimates are correct, most of them do appear to progress. We’re thus forced to rely on inferences from epidemiological studies. Whatever the true number is, given that there are 240,000 new cases of breast cancer diagnosed every year, overdiagnosis is a huge problem, no matter how much some physicians would try to claim otherwise.
Once we acknowledge the existence of overdiagnosis, the questions then become:
- Does the disease found at such an early, asymptomatic stage need to be treated?
- Will treating the disease earlier, before it becomes symptomatic, lead to improved outcomes in terms of survival and/or morbidity?
- Are these early lesions actually cancer?
The answers to these questions are not straightforward in the least, particularly given how difficult it is to show a survival benefit due to early intervention, thanks to lead time bias and length bias. It is this accumulation of evidence of overdiagnosis that has led to a rethinking of cancer screening and changes in recommended screening guidelines. They’re also leading scientists and physicians to reexamine the classification of cancerous-appearing lesions formerly classified as cancer:
In fact, said Dr. Otis Brawley, chief medical officer at the American Cancer Society, the name changes that occurred went in the opposite direction, scientific evidence to the contrary. Premalignant tiny lumps in the breast became known as stage zero cancer. Small and early-stage prostate lesions were called cancerous tumors. Meanwhile, imaging with ultrasound, M.R.I.’s and C.T. scans find more and more of these tiny “cancers,” especially thyroid nodules.
“If it’s not a cancer, let’s not call it a cancer,” said Dr. John C. Morris, president-elect of the American Thyroid Association and a professor of medicine at the Mayo Clinic. Dr. Morris was not a member of the renaming panel.
Dr. Barnett S. Kramer, director of the division of cancer prevention at the National Cancer Institute, said, “There’s a growing concern that many of the terms we use don’t match our understanding of the biology of cancer.” Calling lesions cancer when they are not leads to unnecessary and harmful treatment, he said.
Exactly. It is entirely rational and scientific to adjust medical nomenclature to reflect more recent science and understanding of disease. Again, doing so is anything but simple, as there will always be disagreements, and, yes, turf wars and fears among some physicians who treat these early lesions of losing business, but just because the renaming process is messy and contentious doesn’t mean there is nefarious intent to it or that there was nefarious intent in the nomenclature being replaced.
Reclassifying thyroid cancer
Mr. Ji, of course, is not interested in any of the complexities briefly touched on above. Rather, he is interested in vilifying “conventional” medicine:
Back in 2012, The National Cancer Institute convened an expert panel to evaluate the problem of cancer’s misclassification and subsequent overdiagnosis and overtreatment, determining that millions may have been wrongly diagnosed with “cancer” of the breast, prostate, thyroid, and lung, when in fact their conditions were likely harmless, and should have been termed “indolent or benign growths of epithelial origin.” No apology was issued. No major media coverage occurred. And more importantly, no radical change occurred in the conventional practice of cancer diagnosis, prevention, or treatment.
No major media coverage? Seriously? Besides Medscape, The Wall Street Journal covered it. So did the New York Times. I remember several stories about it in the national media, including television, at the time. Since then, there’s been a lot of coverage of the scientific controversy about overdiagnosis, particularly due to mammographic screening, in the national and international press. Perhaps Mr. Ji’s memory is faulty.
In any case, the summary to which Mr. Ji refers in his introductory rant is this article published in JAMA in 2013 by Laura Esserman (a breast surgeon whose work I admire) and colleagues. It summarized the NCI panel’s recommendations thusly:
- Physicians, patients, and the general public must recognize that overdiagnosis is common and occurs more frequently with cancer screening.
- Change cancer terminology based on companion diagnostics
- Create observational registries for low malignant potential lesions.
- Mitigate overdiagnosis.
- Expand the concept of how to approach cancer progression.
Esserman et al concluded:
The original intent of screening was to detect cancer at the earliest stages to improve outcomes; however, detection of cancers with better biology contributes to better outcomes. Screening always results in identifying more indolent disease. Although no physician has the intention to overtreat or overdiagnose cancer, screening and patient awareness have increased the chance of identifying a spectrum of cancers, some of which are not life threatening. Policies that prevent or reduce the chance of overdiagnosis and avoid overtreatment are needed, while maintaining those gains by which early detection is a major contributor to decreasing mortality and locally advanced disease. The recommendations of the task force are intended as initial approaches. Physicians and patients should engage in open discussion about these complex issues. The media should better understand and communicate the message so that as a community the approach to screening can be improved.
In this light, it is easy to see how utterly silly Mr. Ji’s rant is. The task forces’ recommendations were meant as a starting point for discussion, not a pronouncement. Moreover, one could very much view the reclassification of a variant of thyroid cancer as not being malignant as addressing recommendations #2, 4, and 5. Indeed, this is the first time a lesion that had been classified as a cancer has been reclassified as not cancer.
Let’s take a look at the actual study.
When is thyroid cancer not cancer?
The relevant study, whose first author is Yuri E. Nikiforov, vice chairman of the pathology department at the University of Pittsburgh, basically tells you what you need to know: Nomenclature Revision for Encapsulated Follicular Variant of Papillary Thyroid Carcinoma: A Paradigm Shift to Reduce Overtreatment of Indolent Tumors. There it is right there in the title: This study is addressing recommendations #2 and 4 (at minimum) from the NCI workshop. In fact, it says right in the introduction that that was the purpose of this study! In essence, this paper lays out the case for changing the nomenclature of “encapsulated follicular variant of papillary thyroid carcinoma” (EFVPTC), which is generally treated like thyroid cancer now, to call these lesions “noninvasive follicular thyroid neoplasm with papillary-like nuclear features” (NIFTP). As I’ve discussed before, with the widespread use of thyroid ultrasound, overdiagnosis of indolent thyroid cancers has become a major problem, with large increases in the incidence of these lesions being reported, including noninvasive EFVPTC.
What the authors did was an international, multidisciplinary, retrospective study of patients with thyroid nodules diagnosed as EFVPTC, including 109 patients with noninvasive EFVPTC observed for 10 to 26 years and 101 patients with invasive EFVPTC observed for 1 to 18 years. Noninvasive EFVPTC included EFVPTC that had not invaded through its capsule. Twenty-four pathologists making up the Endocrine Pathology Society working group developed consensus criteria for the diagnosis of EFVPTC, and these were applied to the pathology slides. Molecular analysis of the tumors was also carried out using using ThyroSeq v2, which looks at a panel of 14 oncogenes for mutations.
The authors observed that none of the patients with noninvasive EFVPTC died of their disease in the followup period, while five of the patients with EFVPTC developed metastatic disease and two died. Genetic analysis of the lesions showed that noninvasive EFVPTC was predominately driven by mutations in the RAS oncogene, which are associated with follicular thyroid cancer, as opposed to the mutations in invasive EFVPTC, which were driven by BRAF and RET rearrangements, which have classically been associated with papillary thyroid cancer. On the basis of these observations and a review of the literature the authors recommended their proposed name change and listed rigorous, reproducible diagnostic criteria they propose for differentiating EFVPTC from NIFTP. Because approximately 20% of thyroid cancer is EFVPTC, this name change could affect up to 45,000 patients worldwide per year.
The authors conclude:
The results of this study, together with previously reported observations, suggest that when the diagnosis of NIFTP is made on the basis of careful histopathological examination, the tumor will have a low recurrence rate, likely less than 1% within the first 15 years. Of note, most differentiated thyroid carcinomas relapse within the first decade after initial therapy, although late recurrences and distant spread are documented. Importantly, a large proportion of patients with tumors diagnosed as NIFTP in the present study underwent lobectomy only and none received RAI ablation. This suggests that clinical management of patients with NIFTP can be deescalated because they are unlikely to benefit from immediate completion thyroidectomy and RAI therapy. Staging would be unnecessary. In addition to eliminating the psychological impact of the diagnosis of cancer, this would reduce complications of total thyroidectomy, risk of secondary tumors following RAI therapy, and the overall cost of health care. Avoidance of RAI treatment alone would save between $5000 and $8500 per patient (based on US cost). Decreased long-term surveillance would account for another substantial proportion of cost reduction.
In other words, for this lesion, taking the involved thyroid lobe (or even perhaps just excising the lesion) is probably enough treatment. No completion total thyroidectomy would be necessary, nor would radioactive iodine or followup tests to screen for recurrence. The need for lifelong thyroid hormone supplementation would be eliminated in most patients because they would not require a total thyroidectomy.
Where do we go from here?
As hard as it is to come to a science-based agreement on a set of diagnostic guidelines and a reclassification of a disease entity, where the rubber hits the road will be how these recommendations will be viewed by practicing physicians. It’s reassuring to learn that eight leading professional societies have signed on to the new classification and the new name. That will definitely help with the adoption of the new classification and nomenclature, but it won’t be enough. As I’ve pointed out before, change in medicine is slower than we would like in some areas. We’ve learned that lesson from the Choosing Wisely program, and as the co-director of a statewide quality consortium I’ve learned that implementing change is complex and difficult, and that the wrong kind of change is often too easy to implement.
Practice is also changing to reflect these new realities. For example, men with low grade prostate cancers now often undergo “watchful waiting,” with no intervention unless the tumors progress. (Indeed, I know someone whose treatment involved just that. Unfortunately, he ultimately required radiation therapy, but that was because his tumor progressed.) In breast cancer treatment, recommendations are now less aggressive. For instance, in women over 70 with well-differentiated hormone receptor-positive cancers, radiation is now no longer routinely recommended. Our treatments have become more targeted, as well. For example, there is the OncoType assay that measures the expression of 21 genes to predict whether women with hormone receptor-positive breast cancers with negative lymph nodes require chemotherapy, resulting in less chemotherapy being given. Other assays are also out there.
Indeed, it’s funny how Mr. Ji fails to note that, in this case, Dr. Nikiforov is basically going back to do what Mr. Ji thinks he should do: Let the patients previously treated as though they had cancer know that they didn’t. From a New York Times story on the change:
Dr. Nikiforov says he owes it to patients with reclassified tumors to tell them they never had cancer after all. At the University of Pittsburgh Medical Center, he and others are going to start reviewing medical records and pathology reports to identify previous patients and contact them. He estimates there have been about 50 to 100 each year at the medical center. They no longer have to go back for checkups. They lose the shadow of cancer that the diagnosis hung over their lives.
Informing these patients, Dr. Nikiforov said, “is a moral obligation of doctors.”
Indeed it is. In fact, this reclassification of EFVPTC as NIFTP is arguably the first fruit of the NCI recommendations that Mr. Ji keeps pointing to that actually involved renaming a disease entity. It’s not the first fruit of those recommendations, however. The ACS recommendations for mammographic screening are another. However, renaming disease entities is more difficult in other cancers because the delineation is not so clear-cut. There is no doubt that DCIS can progress to cancer at a substantial rate; the same is true for a lot of other early lesions classified as cancer that might be candidates for a name change, such as prostate cancer. Indeed, when doctors proposed doing just what the NCI proposed for early prostate cancers, there was a great deal of push-back—and not just from physicians. Great care and weighing a huge body of evidence, some of it contradictory, will be required, and it is taking years, as anyone who knew anything about the issues involved in 2012, when the NCI conference occurred, knew it would.
Of course, Mr. Ji isn’t about the careful weighing of evidence. He is about attacking “conventional” medicine and using the “science was wrong before” trope to try to claim that he was right all along and, by implication, he must be right about the “natural” treatments for cancer that he promotes on his website. Even then, he doesn’t understand:
Another topic I have been trying to spread awareness about is thyroid cancer overdiagnosis and overtreatment. When I first reported on this two years ago in my article, Thyroid Cancer Epidemic Caused by Misinformation, Not Cancer, a series of compelling studies from around the world revealed that the rapid increase in diagnoses in thyroid cancer reflected their misclassification and misdiagnosis. As was the case with screening detected breast and prostate “cancers,” and even many ovarian “cancers,” the standard of care often required the removal of the organ, as well as irradiation and chemotherapy — two known cancer promoting interventions.
Actually, overdiagnosis does not involve misdiagnosis. A breast cancer picked up on screening mammography is a breast cancer. Its cells look just as malignant as cells from cancers picked up when a lump forms. The same is true for prostate cancer and, yes, most thyroid cancers. Remember, it’s not just the cancers being reclassified here that are being overdiagnosed by the widespread use of thyroid ultrasound. The real issue is that over the last decade we are learning that many of these cancers are indolent and would never harm the patient if left alone; the problem, of course, is figuring out which are dangerous and which can be either be safely watched or be adequately treated by excision alone. Dr. Nikiforov’s team’s work addresses exactly that question: Which cancers don’t need aggressive treatment? A side benefit of his work is that he identified a variant of thyroid cancer that is so indolent that it basically never metastasizes and therefore shouldn’t be called cancer.
It is useful in these situations to compare alternative medicine to science-based medicine. Those of us advocating for SBM realize its shortcomings better than most, and at least as well as Mr. Ji. We also actively work to change areas where conventional medical care is not adequately science-based. Indeed, this proposed reclassification of a type of thyroid cancer came about because a physician looked at medical practice and saw something not science-based:
The reclassification drive began two years ago when Dr. Yuri E. Nikiforov, vice chairman of the pathology department at the University of Pittsburgh, was asked his opinion about a small thyroid tumor in a 19-year-old woman. It was completely encased in a capsule and the lobe of her thyroid containing it had been removed to establish a diagnosis.
Over the last decade, Dr. Nikiforov had watched as pathologists began classifying noninvasive tumors as cancers and attributed the change to rare cases in which patients had a tumor that had broken out of its capsule, did not receive aggressive treatment and died of thyroid cancer. Worried doctors began treating all tumors composed of cells with nuclei that looked like cancer nuclei as if they were cancers. But this young woman’s story drove Dr. Nikiforov over the edge.
“I told the surgeon, who was a good friend, ‘This is a very low grade tumor. You do not have to do anything else.’ ” But the surgeon replied that according to practice guidelines, she had to remove the woman’s entire thyroid gland and treat her with radioactive iodine. And the woman had to have regular checkups for the rest of her life.
“I said, ‘That’s enough. Someone has to take responsibility and stop this madness,’ ” Dr. Nikiforov said.
It’s doctors like Dr. Nikiforov who see a medical practice that is not adequately science-based and fix it, not quacks like Mr. Ji, whose main interests in cancer seem to be to convince you that chemotherapy kills and causes far more harm than untreated cancer (wrong), that patients with cancer-causing gene mutations don’t need surgery (wrong), and that natural lifestyle changes and whatever supplements he likes can prevent cancer through the magic of epigenetics (wrong again). He latches on to examples like the reclassification of thyroid cancer of SBM correcting itself as evidence that conventional medicine is hopelessly flawed not because he wants to improve medical practice, but because he wants to substitute pseudoscience for science and non-evidence-based “alternative” treatments for validated science-based treatments. Doctors, like Dr. Nikiforov, who promote evidence-based practice are not a validation of Mr. Ji’s profoundly misguided beliefs.
Reclassifying thyroid cancer and the willful misunderstanding of overdiagnosis David Gorski
No comments:
Post a Comment